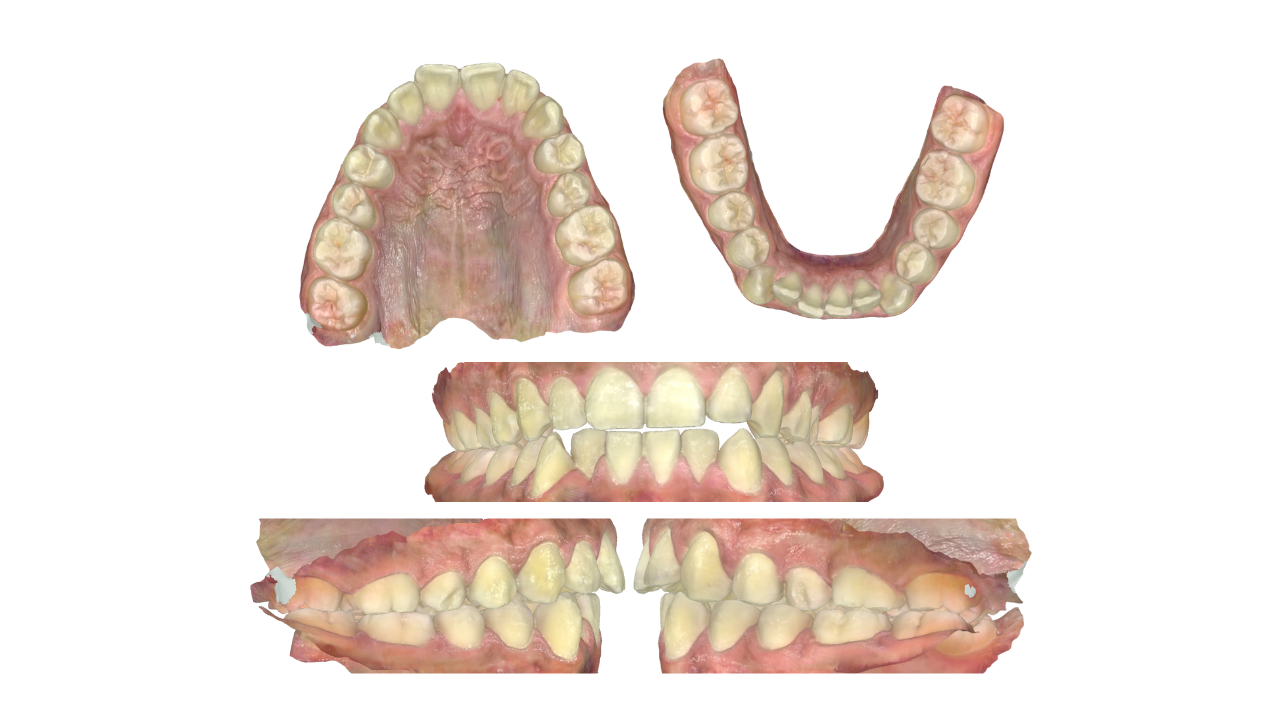
Case 2 - Class 1: Mild crowding, mild anterior open bite, crossbite tendency. Fixed Appliance Plan: Non-Extraction
In this video you'll see a full case walkthrough showing the mechanics I love to use to manage an anterior openbite (AOB) plus how I manage a posterior crossbite tendency affecting the upper second premolars. I'll explain the reasons behind every choice so you can apply good reasoning to your cases. Below you will see a brief summary of the case.
CASE SUMMARY
Diagnosis / Problems List
-
Slight increased vertical, low smile line
-
Incisor C1 (? C2(1))
-
Crossbite tendency U5s
-
Mild (U) + mild/moderate (L) crowding
-
Anterior open bite (1mm)
-
Canines: ¼- ½ C2
-
Incisors proclined (U) + retroclined (L)
-
Overjet increased (7mm)
-
Hypoplastic U5s
Mechanics + Appliances
- Upper and lower fixed appliances
- Class 1 incisor mechanics
- Anterior open bite (AOB) mechanics
- Crossbite mechanics
- Class 2 canine mechanics
Treatment Plan Summary
- Upper and lower fixed appliance
- AOB + crossbite mechanics
- Re-assess for interproximal reduction (IPR) / extraction (XLA)
- Retain
Archwire Sequence
- 014N / 014N
- 18x25N / 018S
- Powerchain U2-2
- 19x25S / 018S
- Powerchain U+L 6-6
- Expand upper wire
- C2 or C3 elastics with a vertical component
- Anterior cross elastic if required
- 018S / 018S
- Powerchain U+L 6-6
- Zigzag settling elastics
- Anterior cross elastic if required
- Debond + Retain
Dr Ib Rominiyi | Orthodontic Specialist & Mentor
Explore all cases in the Ortho Playbook Library
So welcome back to the ortho playbook. Let's get into this case. So this case is a class one case with mild crowding and anterior open bite, and we've got one plan that I'm gonna go through with you. So this patient really wasn't happy about the crowding and mainly in the lower arch. They weren't too bothered about the anterior open bite, and they didn't like the overjet as well. So they were fifteen years old, medically fit and well, no trauma, but they did have a previous digit sucking habit that stopped a few years earlier. Skeletally, they were class one, fMPA was average, the vertical height was slightly increased, not major, Everything else was fine, and the smile line was low. So intraorally, oral hygiene again needs a bit of improvement in that lower labial segment just around here. And in the upper arch they had upper seven to seven present with mild crowding. And in the lower arch they had lower seven seven present with more mild to moderate crowding. And it really depends on where you draw your line, but I would normally go through, the ideal or the best incisors that you like. And I think these these canines are crowded out of the arch. So the incisor classification is between a class one and a class two div one. It's a bit harder to tell when you've got an anterior open by exactly where those lower incisors rest, but it's very close to the cingulum plateau or ever so slightly behind it. The overjet was increased though at seven millimeters and there was a slight anterior open bite. The maximum was about one and a half millimeters between the left lateral incisors. The upper centreline was correct and the lower is basically correct. The canine relationship on the right hand side is about a half class two and the molars are a one. And then on the left hand side the canines are more like a quarter class two, quite similar both of them between a quarter and a half class two. And the molars are a class one on the left. Now there was a slight crossbite tendency on the upper fives as you can see. They're not fully crossbite but that's what you would call a tendency. But there was no displacement. Now in terms of the incisor inclinations, the uppers were proclined and the lobers were retroclined, which is what you would expect with a digit sucking habit. And the occlusal plane was relatively flat, just a normal curve of spin. The main other features are just slight hyperplasia, just these defects on these upper fives, ever so slightly on the four but mainly on the fives which might affect bonding, it might not. I would just warn the patient I think it should be okay. The OPT shows all teeth present, no pathology, normal bone lengths, bone height and root lengths. So that all looked fine and the wisdom teeth developing. The problem list, this is my standard problem list I use to make sure I don't miss anything when I'm diagnosing PET cases. For this patient, their diagnosis will be a slight increased vertical proportions extraorally and a low smile line. The incisors were class one, maybe slightly class two to one. The overjet was increased to seven millimeters. The crossbite tendency on the fives, mild upper and mild to moderate lower crowding, an anterior open bite between one to one point five millimeters, the canines about a quarter to a half class two and the upper incisors are proclined whilst the lowers were retroclined and just a slight hyperplastic upper fives. OPT showed no pathology. So the treatment aims, again, are my standard treatment aims that I use to when I'm trying to aim for an ideal occlusion, just achieving excellent oral hygiene. I'm gonna relieve all the crowding. Gonna level and align the arches. I'm going to correct. My aim is to correct the overbite, and I'm aiming to achieve class one canines. I wanna maintain full unit molars, and I wanna achieve class one incisors with an average overjet and average inclination. I want to maintain the coincident centerlines, the matching centerlines, and I wanna coordinate the arches, so correct those slight crossbite tendencies. I wanna close any residual spaces, do finishing and detailing, and then finally retain all of those changes. Next is my gearbox. So this is the simple framework that I use to hack orthodontic decision making, and it's the questions I ask to find the mechanics that I need to build a plan that I can trust. And it's in the same order and as my treatment aims. This is the order that I usually treat most cases. So what am I gonna do to relieve the crowding? For this, in the upper arch, definitely non extraction. In the lower arch, I'm gonna reassess for extraction because there might be need just for IPR or extraction potentially of one lower incisor or the lower five because the crowding is on the mild to moderate side. It's one that I would definitely attempt to manage non extraction, see if I can get away with it, see if we can squeeze them all in. And the main thing that I'm monitoring is recession. If you try and align everything, everything comes further forwards. If you push it too far out of the bone, you get a bit of recession. You might be able to tuck it back in with some IPR. It might be too severe that you need extraction of an incisor or the lower fives. I don't think you need the fours. That will give you too much space. Then next, level and align the arches. What am I gonna do to do that? So I think my standard aligning arch wise would be sufficient, and I wanna tie this in as much as possible. So for that, I would usually tie in the most displaced teeth first, like that lateral incisor and this lateral incisor, because that's when the wire is the most flexible. And then I'll tie in the additional teeth. And to start off with, I might just start off with partially tying them in if I can't tie it in fully. And then as a t straighten up a bit, the next visit I'll tie them in fully with like figure of eight ligatures. I would also use lace backs in this case and I would use them in the lower quadrants and that's because I've got quite a bit of anterior crowding. And what the lace backs are gonna do is it's just gonna hold these canines back. It fixes the distance between your molars and your canines because we know the canines have got the greatest degree of mesial tip. The canines wanna tip forwards because that's in an ideal position. That's where they would be. But that is just gonna encroach on this, incisor space, which is already crowded. I don't want them to come any further forward. So I gotta hold them, give my incisors a bit of breathing room, let them align up, and then let go once the incisors are lined up. So I'll do the lace backs definitely in the lower quadrant for that reason. Then in terms of the overbind. Now I'm gonna use my AOB mechanics. So I'm gonna stay in a lower round arch wire, so an o one eight stainless steel arch wire, arch wire. And I'm gonna do some vertical elastics. So I want vertical force, and I want it to be anterior, not posterior. And there's loads of different options that you would do, and I'll probably do a combination of some of these. But if I ever needed any class two elastics, which you might do for this case, I would make sure there's a vertical component to that. Another option is an anterior elastic that can go around the incisors or the canines or combination. Then you've got an anterior v elastic. So example, from upper four to lower four to upper three. And that's just this v shape that just helps give a vertical force anteriorly or an inverted beam. So that can be from the lower lower four to the upper three to the lower three. Again, a bit more anterior, but it's just to close that down there. And then finally, I would reassess for extractions. Now with an anterior open bite, you wanna if you are gonna extract, you prefer to extract further back because of the wedge shaped effect. It's gonna help close this down. So I'll consider all the fives. Now for my canines, how am I gonna get them to class one? Or, again, in this case, I might accept a slight class two because I'm prioritizing my incisors. So adaptive class two canine mechanics. So I would consider accepting the class two mainly because this could be a class three case. Once these align forwards, these incisors could end up slightly class three, and the overjet is a priority. And so in those cases, I would want the incisors to be have a positive overjet, and so I don't mind if the lower arch goes back a little bit and the relationship for the canine is slightly class three class two. Sorry. So in this case, I would probably avoid class two elastics to get the canines back because I just think it's gonna move everything closer to a class three. Once these incisors align, they're gonna come forwards, and I could risk a reverse overjet, so I probably would avoid that. And instead, I would do inverted v elastics. So from the lower four to the upper three down to the lower three to try and get these into a class one relationship as close as possible. And I would reassess for IPR, and that would be distal to the upper three, so let these canines come back, and mesial to the lower three, so let the canines come forwards. Remember, the main reason why we want to get our canines to class one is because it helps us get our incisors to class one. That's the main reason. So that's why you would adapt it if you need to prioritize incisors. And then finally, I would reassess for extraction, and I would consider one lower incisor, which would help bring these canines forwards, get them to class one, also help with the reverse overjet, or all of the fives. That's another option. And then the molars. Now they're class one. I would expect them to remain class one, so I would just keep that under review. And then for the incisors, now I would expect a class one finish if we're careful, once these incisors come forwards. And so I would work to an upper nineteen twenty five stainless steel and a lower o one eight stainless steel. Now remember, we're doing the o one eight stainless steel for the overbite for the AOB mechanics. But staying in an o one eight stainless steel would also help us if we ended up a little bit class three because we're the class three mechanics. I would run power chain six to six to retract the site inside if there's any space and reassess for IPR, and I'm thinking it's mainly gonna be in the lower arch that we'd be doing that. I would closely monitor the overjet and I would use class two or class three incisor mechanics if required to elastics. So my class two or class three elastics, if these all lined up and we did quite a lot of IPR to get them aligned, you might end up with an increased overjet. So you might end up more class two, and so you do some class two elastics and you'll be fine with that. If not, if we these were a bit more per client, came a bit forward, you could end up with class three, and so I would do some class three elastics. Now if the overjet was increased, I would my class two mechanics, I would use a smaller arch wire. So instead of going up to a nineteen twenty five steel in the upper, that's gonna per climb these incisors, I would go to an eighteen twenty five steel or a sixteen twenty two steel, which can just let these become a little bit more upright with the power chain and the elastics. If you ended up edge to edge or a bit class three or a reverse overjet, then I would do my class three elastics and just stay in that lower o one eight stainless steel arch wire, which is great, which we're already doing. But I would also swap the lower three brackets. So I would swap the left and right lower three brackets because the lower canines, they want to procline or tip nasally. And if you swap them left and right, that's just gonna make them tip distally, and it's gonna help everything go a little bit further back so you get a positive overjet. That's the priority. In this, I think if we're careful, we can get class one. So the centerline, just my standard, centerline mechanic. So if that's off slightly, I would just do an anterior quad elastic if required and maybe some IPR. And for the crossbite, the buccal crossbite tendency, would use buccal crossbite mechanics. So in the upper arch, I would expand the arch wires when I get stainless steel, get them really big, and then tie them in, and that's gonna wanna bring the teeth out. And, again, in the lower arch, I'll stay in an o one eight stainless steel arch wire. So there's loads of reasons to stay in the lower round arch wire for this case, but that's gonna also help these lower arch teeth just to roll in lingually, especially with the power chain, and let the upper arch be wider so we get a correct crossbite. We correct the crossbite. Then my finishing would just be standard finishing. Upper and lower o one eight stainless steel arch wires, do any repositioning or finishing bends. Power chains, six to six if any space, zigzag elastics, and the anterior cross elastic if required. And then just debond with retainers. So let's look at the plan. So number one, as standard, leave and monitor. Number two, open lower fixed appliances. Reassess for IPR or extraction. I think there's a good chance we would definitely need IPR, maybe extraction, and then retain. And the main risks, additional risks for this case are the risks of an anterior open back, an AOB, and so I would use my AOB mechanics. So let's look at this step by step for this plan. So I would start off with upper and lower o one four night high, and I would probably just bond all of the teeth. I will put lace backs in the lower quadrants, and I will tie in this lateral incisor first. I would do my posterior bite blocks, so composite or GIC on the upper sixes, if required, or bite raising modules, which I don't think you would need in this case. And I'd retie until it's passive. Tie an o one six night tie if needed, but I don't think I would need to. I will just move straight on to the next stage. So for me, that would be an upper eighteen twenty five night time and a lower o one eight stainless steel arch wire. And at this stage, I would actually start off with some anterior vertical elastic, start managing the overbite. So it's alignment and overbite at this stage. If there's any space, I always do power chain upper two to two at this stage. And my vertical elastics anterior probably would go for this inverted v. So from the lower four to the upper three to the lower three, or I would do an anterior box elastic, either or. I think patients probably might prefer this than the box, and I'd get them to wear it as much as possible, ideally full time. But they won't be able to eat with it in so they'll have to take it out for eating. And then I would move on to my nineteen twenty five steel in the upper and keep my o when I stay in the steel in the lower. So these are my main working archbires now. And the focus on this is also to correct the overbite, but at the canines, incisors, and molars, we're trying to correct these all as well. So if there's any space, would do power chain six to six. I don't really expect there to be any space. And I would do my inverted v elastics again. So not only did these help with the overbite, but it's also gonna help get these canine to class one, which I'd want as well. And as the teeth align up, I think these incisors are gonna get closer to class one. There is a risk that they might be a bit class three, so we'll keep an eye on that. So if they are, then we would consider our class two or class three elastics with the vertical component. So if it's class three, it would go from the upper six down to the lower three up to the upper three. And if it's a class two, it would go from the lower six to the upper three down to the lower three. Just depending on how much IPR we needed to get these teeth straight. And that would depend determine the risk of it being class one, class two, or class three finish. So, again, like this, that's how it could look for the class two. So I would also do the anterior quad elastic if I needed to at this point just to keep those center lines matched up. Again, that can go from the upper three to three or two to two if you've got some Kobayashi hooks on. And I'd reassess for IPR and extractions, really looking about recession. If I was able to get all the teeth in when I'm looking for a recession to see if we've pushed it out too far, it may well be that they just don't line up and then you need some IPRs to get them aligned or you need to extract before we even get to this stage. And then I would finish. And I would finish with upper and lower o one eight stainless steel arch wires and power chain six to six, zigzag elastics, and anterior cross elastic. And I would consider an anterior box if you still needed to because when you've got an anterior open bite, often once that has even been corrected, you kinda still want to maintain it even just at night times only. So when you're starting to correct it, you want all of the vertical anterior forces full time or as close to full time as the patient can tolerate. And then later on, you would just drop down to nine times only just to maintain it. So that's what I would consider with that one if it opens up again later on. And then I would debond and finish with my retainers as standard. And so that's how I would manage this case. Speaker 1: ... Speaker 2: ...Click to read the full transcript